Table of Contents
USP <659>: Packaging and Storage Requirements for Pharmacy Teams
USP <659> packaging and storage requirements may not get the same attention as USP <795>, <797>, or <800>, but they affect one of the most common pharmacy compliance workflows: making sure medications are stored, protected, monitored, inspected, and handled according to their labeling and intended conditions.
For pharmacy leaders, USP <659> is not just a chapter about containers or temperature words. It provides important vocabulary for packaging, storage conditions, and medication protection. Those definitions can influence pharmacy policies, temperature monitoring programs, unit inspection forms, medication room expectations, refrigerator and freezer alarm settings, and temperature excursion response.
In the Pharmacy Compliance Alphabet Soup series, USP <659> belongs in the storage, packaging, distribution, and medication management conversation. It connects the pharmacy, nursing units, clinics, procedural areas, home infusion operations, specialty pharmacy shipping, and any other setting where medications may be stored outside the central pharmacy.
What Is USP <659>?
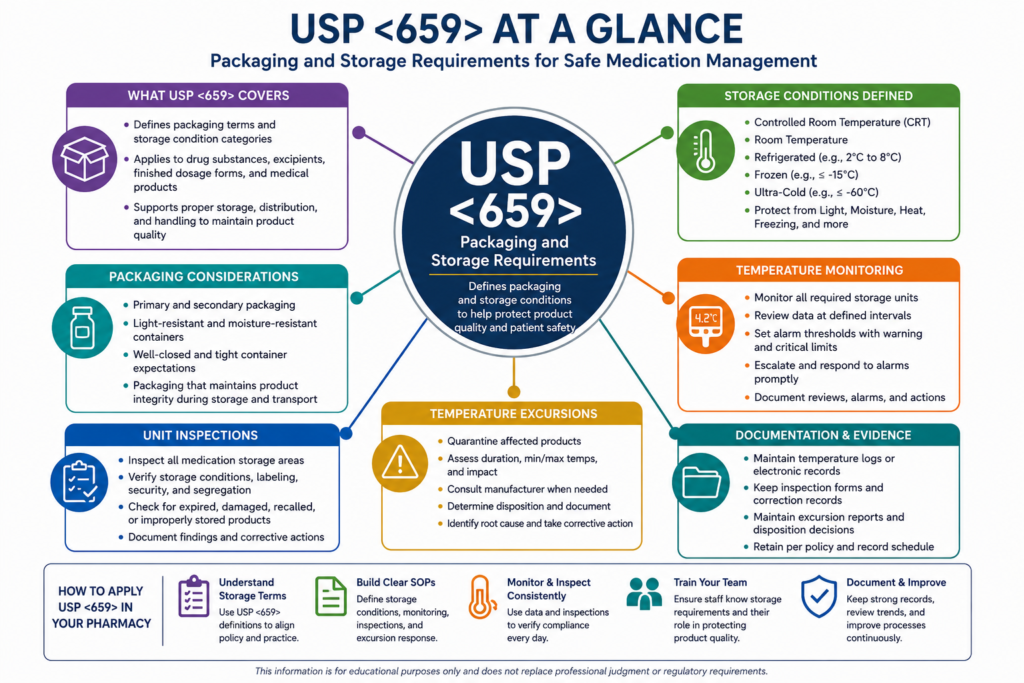
USP General Chapter <659>, Packaging and Storage Requirements, provides packaging definitions, auxiliary packaging information, and storage condition definitions relevant to the storage and distribution of drug substances, excipients, medical products, and other articles covered by USP. USP describes the purpose of the chapter as providing packaging and storage condition definitions for products such as pharmaceuticals, combination products, and related medical products.
In practical terms, USP <659> helps pharmacy teams answer questions such as:
What does “room temperature” mean in our medication storage policy?
How should we interpret “refrigerated,” “cold,” “freezer,” or “protect from light”?
What should be protected from moisture, excessive heat, freezing, or light?
How should storage language on a manufacturer label translate into monitoring, documentation, and response?
What evidence should we maintain when a medication storage area is inspected?
USP <659> should not be read in isolation. It often works alongside product labeling, USP monographs, state board of pharmacy rules, accreditation standards, manufacturer instructions, CDC guidance for vaccines, and internal health-system or pharmacy policy. USP <1079> and related storage and distribution chapters can also support broader risk mitigation, temperature monitoring, transport, and distribution practices. USP notes that proper storage and transportation of finished drug products are critical activities in an integrated supply chain.
Why USP <659> Matters for Medication Management
Medication management is not limited to prescribing, verifying, dispensing, and administration. It also includes maintaining medication integrity before a dose ever reaches the patient.
A pharmacy can have strong clinical review processes and still create risk if medications are stored in the wrong area, exposed to heat, left in an uncontrolled refrigerator, stored in a location without routine inspection, or returned to stock after an undocumented excursion.
USP <659> supports medication management by helping teams standardize the language of storage. That language then becomes operational in policies, task lists, inspection tools, staff training, and corrective action workflows.
For example, a hospital pharmacy may need to confirm that medications stored in automated dispensing cabinets, anesthesia carts, crash carts, clinic refrigerators, procedural areas, and nursing unit medication rooms are kept under appropriate conditions. A retail pharmacy may need to monitor will-call bins, vaccine refrigerators, room temperature shelves, quarantine areas, and delivery staging areas. A specialty or home infusion pharmacy may need to connect storage requirements to packing, transport, courier expectations, and patient delivery documentation.
USP <659> and Unit Inspections
Unit inspections are one of the most practical places where USP <659> becomes visible. For hospitals, health systems, clinics, and long-term care settings, medication storage does not stop at the pharmacy door. Medications may be stored across dozens or hundreds of locations.
A comprehensive unit inspection program should evaluate more than whether medications are expired. It should help confirm that storage conditions, labeling, security, segregation, and documentation match policy.
A USP <659>-informed unit inspection may include review of:
Medication storage temperatures for refrigerators, freezers, warmers, and room temperature areas.
Evidence that storage units are monitored and that temperature logs or electronic records are reviewed.
Expired, damaged, recalled, discontinued, or unlabeled medications.
Medications stored outside approved locations.
Look-alike/sound-alike or high-alert medication segregation.
Light-sensitive medications stored according to labeling.
Products requiring protection from freezing, heat, moisture, or light.
Open-vial, short-dated, or punctured container dating.
Emergency medication carts, trays, kits, and anesthesia storage.
Quarantine processes for medications affected by temperature excursions or storage concerns.
The goal is not to create a checklist for the sake of a checklist. The goal is to create a repeatable evidence trail showing that medication storage areas are routinely reviewed, findings are corrected, and trends are escalated when needed.
Temperature Monitoring: From Storage Words to Operational Controls
USP <659> gives pharmacy teams a vocabulary for storage conditions, but pharmacy leaders still need to translate that vocabulary into operational controls. That means clearly defining temperature ranges, aligning those definitions with authoritative sources, and ensuring staff understand exactly what those ranges mean in practice.
One of the most common areas of confusion is the difference between general “room temperature” and USP-defined “controlled room temperature.” In USP terminology, controlled room temperature typically refers to a range of 20°C to 25°C (68°F to 77°F), with allowable short-term excursions between 15°C and 30°C (59°F to 86°F). However, other organizations may use the term “room temperature” differently. For example, OSHA or general workplace standards may consider room temperature in broader comfort-based ranges that are not appropriate for medication storage. Manufacturer labeling may also use “room temperature” without explicitly stating whether it aligns with USP definitions.
Because of these differences, pharmacy teams should avoid assuming that all references to “room temperature” are interchangeable. Policies should explicitly define what temperature ranges apply to medication storage and should reference USP definitions, manufacturer labeling, and any applicable regulatory or accreditation requirements. Without this clarity, teams risk inconsistent monitoring, incorrect alarm settings, and potential product integrity issues.
A strong temperature monitoring program should identify:
Each monitored storage location.
The products stored in that location.
The required storage range based on labeling and policy.
The monitoring device used.
The alarm thresholds.
The notification pathway.
The response timeframe.
The quarantine and release process.
The documentation record.
The escalation pathway if the issue repeats.
This is where pharmacy teams should be especially careful. Alarm settings and monitoring ranges should not be copied casually from a generic template. They should be based on the most restrictive applicable requirement, including manufacturer labeling, USP terminology, CDC guidance for vaccines, state board expectations, accreditation standards, and facility policy.
Clearly defining temperature ranges is not just a documentation exercise. It directly impacts how alarms are configured, how excursions are identified, and how staff respond in real time. If ranges are poorly defined or misunderstood, teams may either overreact to non-events or, more concerning, fail to recognize true excursions that could compromise medication quality.
What Temperature Alarm Levels Should Pharmacies Set?
A practical rule is this: do not set alarms only at the point where the storage condition has already failed. Use internal warning thresholds that give staff time to respond before an excursion occurs.
For refrigerated medications labeled for 2°C to 8°C storage, a pharmacy might use warning alerts before the outer limits, such as around 3°C on the low side and 7°C on the high side, with critical alarms at or near the labeled limits of 2°C and 8°C. For vaccines, CDC states that vaccines licensed for refrigerator storage should be stored at 2°C to 8°C, or 36°F to 46°F. CDC’s Vaccine Storage and Handling Toolkit also references common ranges of 2°C to 8°C for refrigerators, -50°C to -15°C for freezers, and -90°C to -60°C for ultra-cold freezer storage.
For frozen medications, alarm settings should reflect the product’s labeled range. A vaccine freezer range may be different from a medication freezer range, a biologic freezer range, or a product-specific ultra-cold storage requirement. For room temperature storage, teams should verify the current USP definition, product labeling, and policy before setting thresholds. Controlled room temperature language, permissible excursions, and manufacturer instructions may not all mean the same thing in every situation.
A practical alarm framework may include:
A warning alert before the range is exceeded.
A critical alarm at the policy or labeled boundary.
An after-hours escalation pathway.
A repeat alarm escalation if the same unit alarms multiple times.
A power failure response process.
A documentation requirement for all alarm review and resolution.
This approach helps avoid the common problem of discovering an excursion only after product storage conditions have already been compromised.
Temperature Excursions: What Should Happen Next?
When a temperature excursion occurs, the most important first step is to protect the product while the situation is evaluated. Staff should not assume products are usable, discard products prematurely, or return items to active inventory without review.
A defensible temperature excursion workflow should include:
Identify the affected storage unit and products.
Record the date, time, duration, minimum temperature, maximum temperature, and current temperature.
Move products to a stable, appropriate storage location if needed.
Clearly quarantine affected inventory.
Do not use affected products until disposition is determined.
Contact the manufacturer or appropriate authority when needed.
Document the final decision and who made it.
Perform corrective action if the root cause suggests a process, equipment, or staff training issue.
Trend repeated events.
For vaccines, CDC emphasizes that improper storage can reduce potency and that potency, once lost, cannot be restored. CDC also notes that exposure to freezing temperatures can permanently affect certain vaccines. This concept matters beyond vaccines: temperature excursions are not just documentation events. They are product integrity events.
Packaging, Light Protection, Moisture, and Storage Integrity
USP <659> is also about packaging. Packaging matters because a container or closure system can affect whether a medication remains protected from light, moisture, contamination, evaporation, adsorption, or other quality risks.
Pharmacy teams should consider packaging and storage together when reviewing:
Original manufacturer containers.
Repackaged medications.
Unit-dose packaging.
Compounded preparation containers.
Light-resistant packaging.
Tight or well-closed container expectations.
Medication bins and transport totes.
Emergency kits and trays.
Automated dispensing cabinet pockets.
Patient-specific delivery packaging.
For example, a light-sensitive medication may be stored correctly in the central pharmacy but become noncompliant if it is removed from protective packaging and placed in an open medication bin. A medication requiring protection from moisture may be compromised if repackaged or stored in a way that does not maintain the intended barrier. A refrigerated product may be placed in an appropriate refrigerator but still be at risk if staff leave it staged at room temperature during receiving, delivery, or return-to-stock workflows.
How USP <659> Relates to Compounding and IV Workflow
USP <659> is especially relevant for compounding pharmacies and health-system IV workflow teams because storage and packaging influence beyond-use dating, labeling, handling, transport, and release processes.
For compounded preparations, pharmacy teams should connect storage requirements to:
Master formulation records.
Compounding records.
Container selection.
Final preparation labeling.
Beyond-use dating rationale.
Light protection requirements.
Refrigerated, frozen, or room temperature storage instructions.
Transport from pharmacy to patient care area.
Return-to-stock or return-to-inventory rules.
Temperature excursion response.
For sterile compounding, storage is also tied to workflow controls. If a compounded sterile preparation is labeled for refrigerated storage, pharmacy teams need evidence that the product was stored appropriately from preparation through dispensing or administration. If a preparation moves from one storage condition to another, teams should understand whether that affects the BUD, labeling, or use instructions.
Building a USP <659> Informed SOP
A practical USP <659> informed SOP should be clear enough for daily users and detailed enough for inspection readiness. It should define storage categories, monitored areas, responsibility, documentation, alarm response, excursion handling, and corrective action.
A strong SOP may include:
Purpose and scope.
Definitions for storage conditions.
Medication areas covered by the policy.
Roles and responsibilities.
Receiving and stocking expectations.
Room temperature storage expectations.
Refrigerator, freezer, and ultra-cold storage expectations.
Medication warmer expectations, if used.
Packaging and light-protection requirements.
Unit inspection process.
Temperature monitoring process.
Alarm threshold logic.
Excursion response process.
Manufacturer consultation process.
Quarantine and release documentation.
Corrective action and trend review.
Staff training expectations.
Record retention expectations.
The SOP should also clarify that product labeling and manufacturer guidance may override general assumptions. If a medication has specific storage instructions, those instructions should drive the operational control.
How Pestle Can Help
Pestle can support pharmacy teams by helping standardize recurring compliance work tied to medication storage, unit inspections, temperature monitoring, and excursion response. Instead of relying on disconnected spreadsheets, paper binders, or informal reminders, teams can use Pestle to organize assigned tasks, document completion, track findings, and maintain evidence over time.
For example, a pharmacy team could use Pestle Compliance to schedule monthly unit inspections, assign refrigerator log reviews, document temperature excursion follow-up, and organize corrective actions. A compounding team using Pestle Formulas can also benefit from more standardized preparation records, labeling information, storage instructions, and workflow visibility.
Pestle is designed to support pharmacy compliance operations, but it does not replace professional judgment, regulatory interpretation, legal guidance, manufacturer consultation, or pharmacy policy review. Teams should validate their USP <659> workflows against their practice setting, state requirements, accreditation program, product labeling, and internal procedures.
Pestle Compliance
Pestle Formulas
USP Chapters Explained: Beyond USP <795>, <797>, and <800>
Conclusion
USP <659> may look like a packaging and storage definitions chapter, but for pharmacy teams it has broad operational impact. It helps shape how medications are stored, how temperature ranges are interpreted, how unit inspections are structured, how alarms are configured, and how temperature excursions are documented.
The most effective pharmacy programs treat medication storage as a medication management process, not a facilities afterthought. That means connecting USP language, product labeling, monitoring devices, inspection tasks, alarm response, quarantine workflows, and corrective action into one repeatable system.
For pharmacy leaders, the practical question is not simply, “Do we know what USP <659> says?” The better question is, “Can we prove that our storage practices match our policies every day, in every medication storage location?”
Pestle can help pharmacy teams turn that question into a structured compliance workflow that is easier to assign, document, review, and improve over time.